

Sustained testosterone
suppression to <50 ng/dL1
96.7%
(95% CI: 94.9-97.9)88.8%
(95% CI: 84.6-91.8)*†Non-inferiority assessment between treatment groups was not accepted by FDA due to different censoring rules in historical trials.2
HERO Study Design
The efficacy and safety of ORGOVYX were evaluated in a multinational, phase 3, randomized, open-label, parallel-group study1,3,4

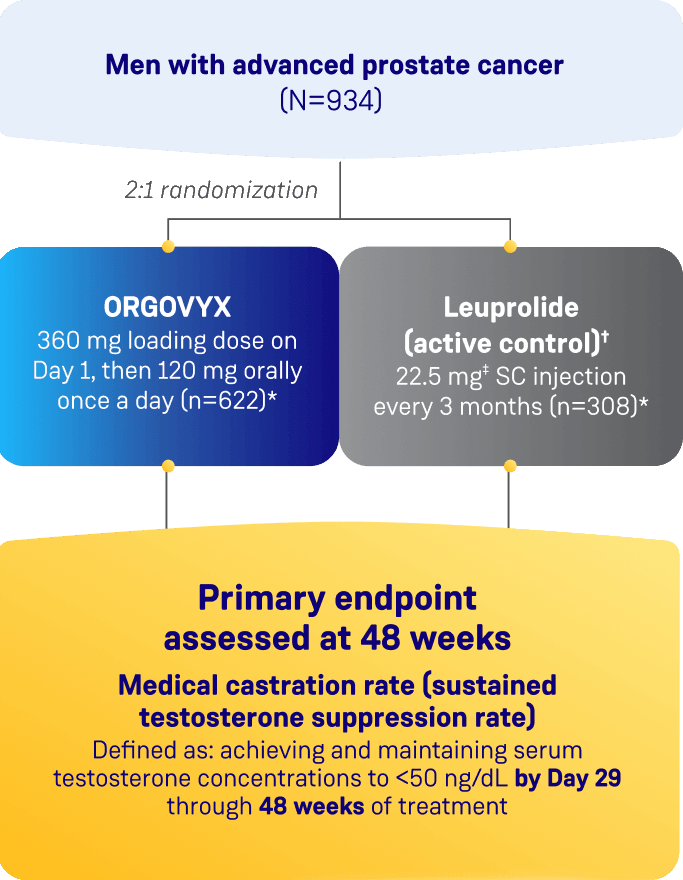
Two patients in each arm did not receive the study treatment and were not included.1
Patients randomized to leuprolide acetate could receive an antiandrogen.4
The dosage of leuprolide was 11.25 mg in Japan and Taiwan, per local guidelines, and is not recommended for prostate cancer in the United States.1
ECG=electrocardiogram; SC=subcutaneous.
- Testosterone suppression rates on Day 4 and Day 15 (defined as testosterone concentrations <50 ng/dL)
- Profound testosterone suppression rates on Day 15 (defined as testosterone concentrations <20 ng/dL)
Mean change in PSA—Change in PSA levels on Day 15 (≥50% decrease from baseline), confirmed on Day 29. In the HERO study, change in PSA levels was prespecified to be monitored monthly. The therapeutic effect of ORGOVYX should be monitored by measuring serum concentrations of PSA periodically. If PSA increases, serum concentrations of testosterone should be measured.
No evidence has shown that the rapidity of PSA decline is related to a clinical benefit.
Testosterone recovery substudy—Cumulative probability of testosterone recovery above the lower limit of the normal range (>280 ng/dL) or baseline at the 90-day follow-up in a subset of patients who completed 48 weeks of treatment and who did not receive subsequent ADT for at least 90 days after discontinuation.
This endpoint was analyzed for exploratory purposes without formal testing.
ADT=androgen deprivation therapy; PSA=prostate-specific antigen.
Efficacy Data
ORGOVYX achieved sustained testosterone
suppression to <50 ng/dL1
- 96.7% of men achieved and maintained testosterone suppression to <50 ng/dL from Day 29 through Week 48 with ORGOVYX
Sustained testosterone suppression rate
(Testosterone levels <50 ng/dL from Day 29 through Week 48)1
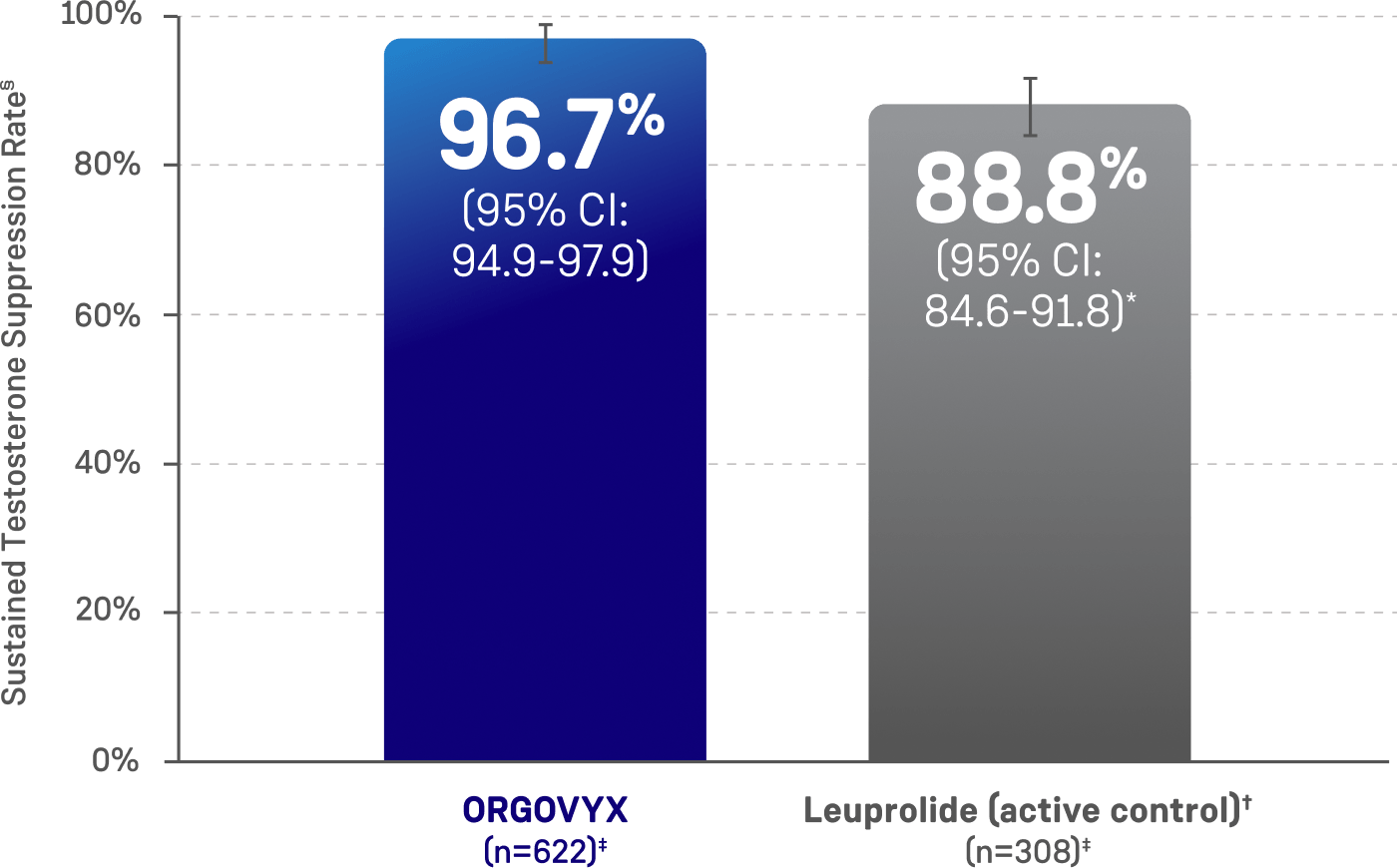
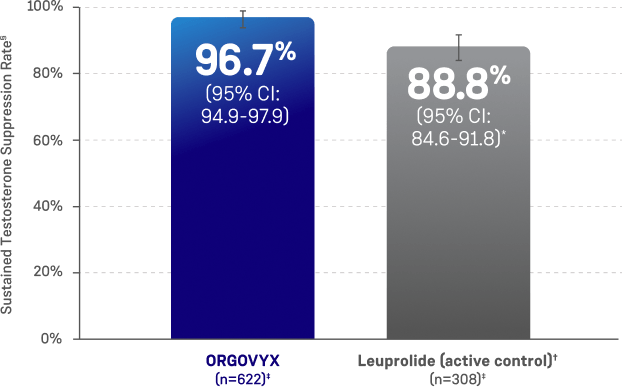
There was no statistical testing between the two treatment groups and comparisons cannot be made.
11.25 mg is a dosage regimen that is not recommended for this indication in the US. The castration rate of the subgroup of patients receiving 22.5 mg leuprolide (n=264) was 88.0% (95% CI: 83.4%, 91.4%).1
Non-inferiority assessment between treatment groups was not accepted by FDA due to different censoring rules in historical trials.2
Two patients in each arm did not receive the study treatment and were not included.1
Kaplan–Meier estimates within group.1
CI=confidence interval.
Rapid testosterone suppression
sustained throughout the HERO study1,3
Percentage of patients attaining testosterone decreases to
<50 ng/dL within the first 29 days in HERO1*
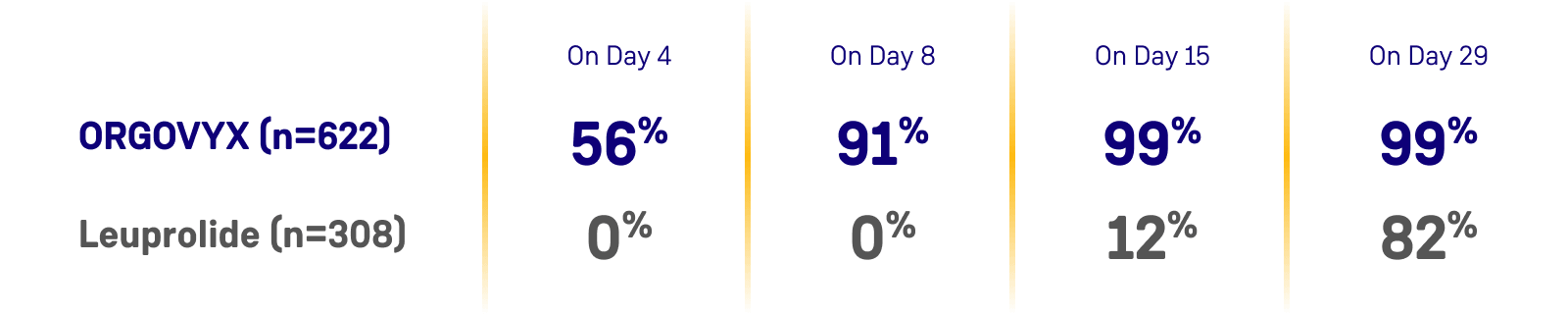
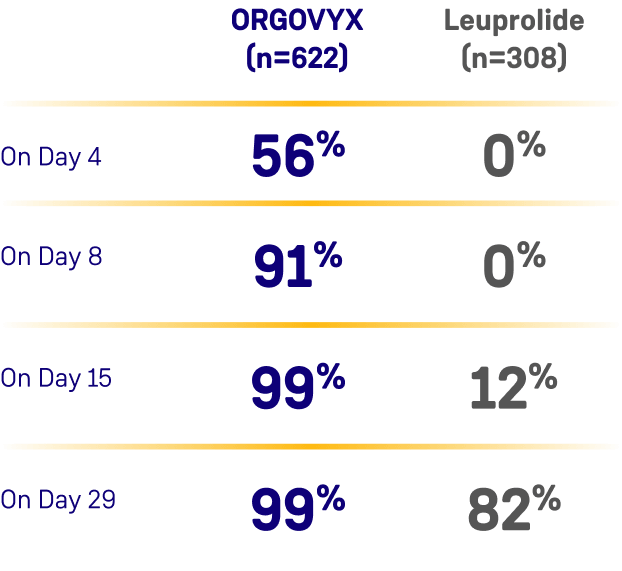
*Kaplan-Meier estimates within each group.1
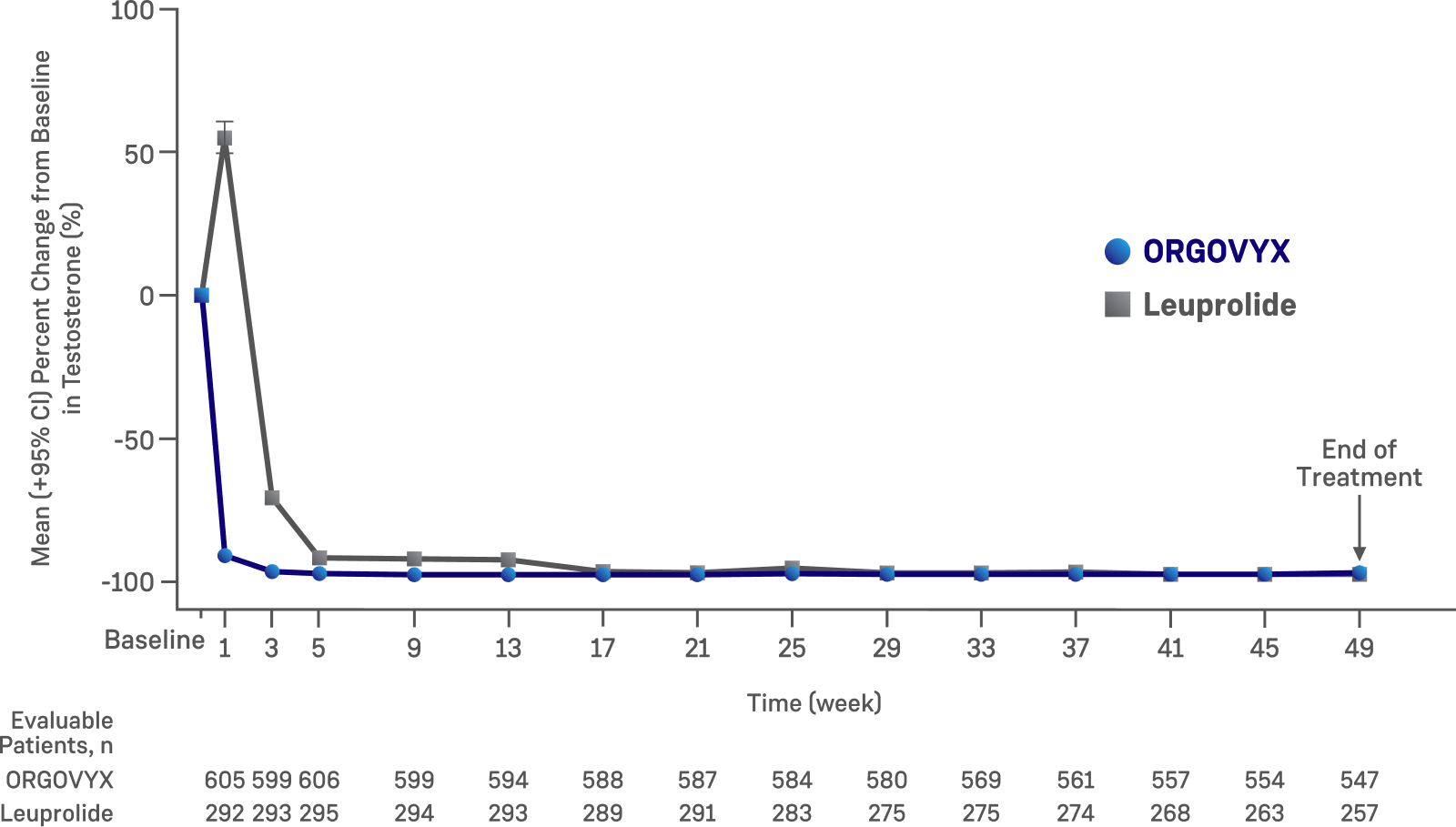
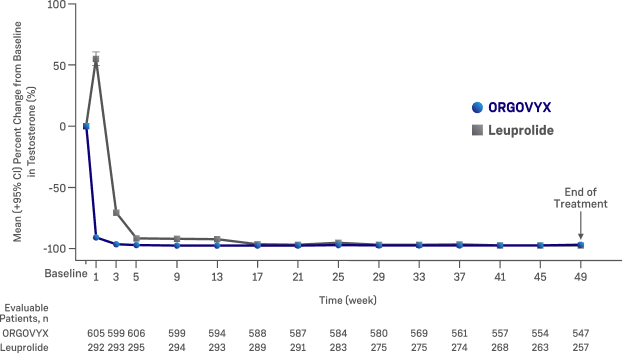
Mean (95% CI) percent change from baseline in testosterone
concentrations from baseline to Week 49 by treatment group in HERO1
Profound testosterone suppression
On Day 151:
- 78% of men treated with ORGOVYX achieved profound testosterone suppression to <20 ng/dL
- 1% of men treated with leuprolide achieved profound testosterone suppression to <20 ng/dL
Percentage of patients attaining testosterone decreases to
<20 ng/dL within the first 29 days in HERO1*
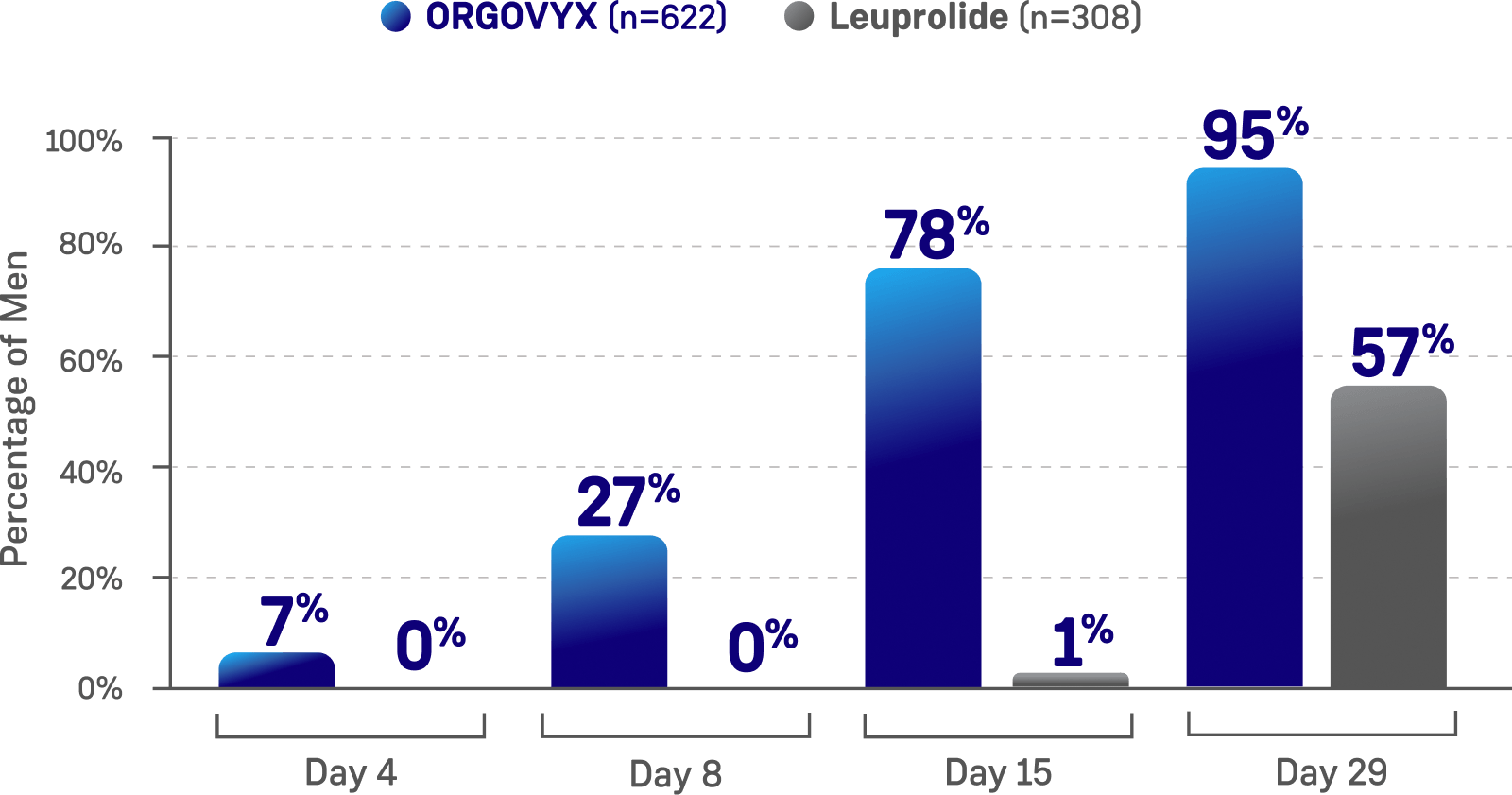
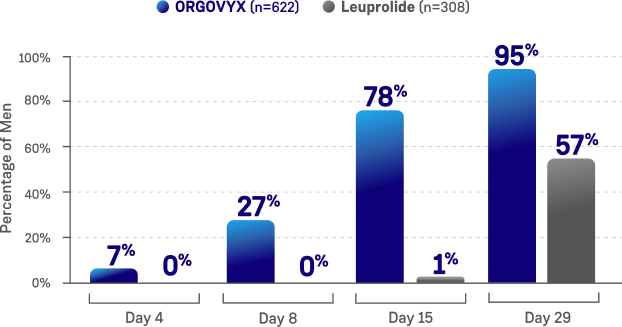
*Kaplan-Meier estimates within each group.1
ORGOVYX lowered PSA levels
In HERO, PSA levels were prespecified to be monitored and measured at baseline (Day 1) and remeasured at each visit (eg, Week 2, Week 4, Month 3, Week 48)1,3
This endpoint was analyzed for exploratory purposes without formal testing.1,3
These PSA results should be interpreted with caution because of the heterogeneity of the patient population studied.
No evidence has shown that the rapidity of PSA decline is related to a clinical benefit.1,3
PSA levels were lowered on average by 65% two weeks after administration of ORGOVYX, 83% after 4 weeks, 92% after 3 months and remained suppressed throughout the 48 weeks of treatment1,3
Reductions in PSA levels in men with an average starting PSA of 104.2 ng/mL (N=622)1,3
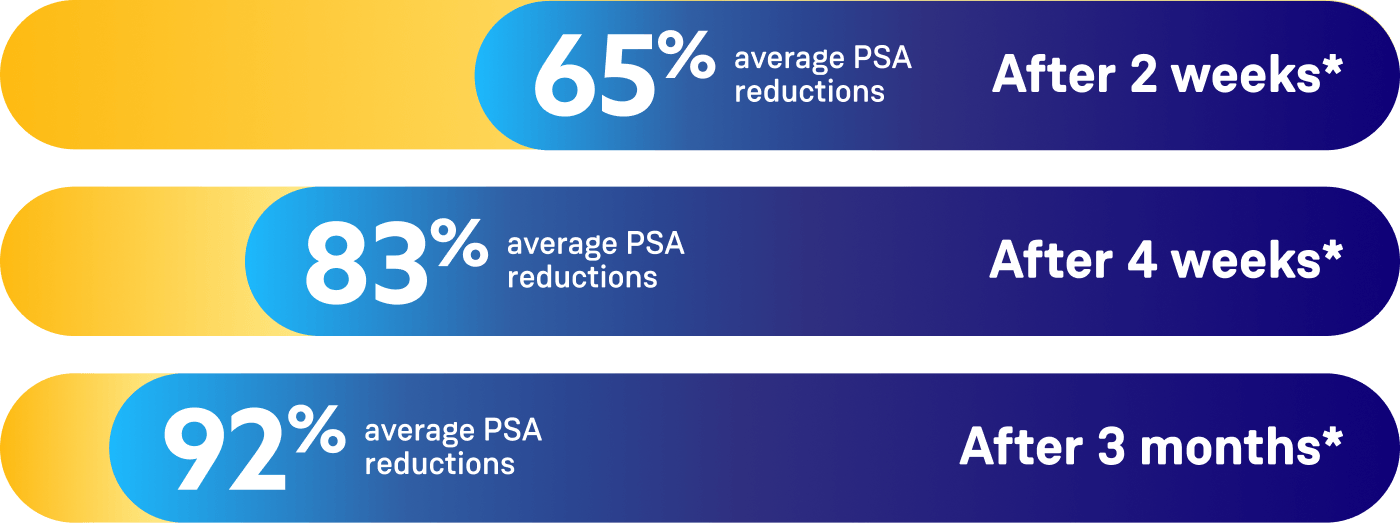
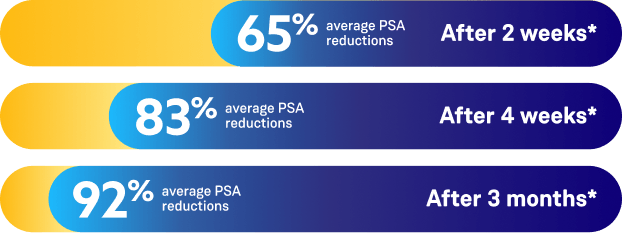
Percentages are based on patients who had PSA results available at each time point. Percentages reflect mean percent change across patients with an evaluable PSA at that visit.
The therapeutic effect of ORGOVYX should be monitored by measuring serum concentrations of PSA periodically. If PSA increases, serum concentrations of testosterone should be measured.1
Testosterone recovery 90 days after
treatment discontinuation1,3,5
The testosterone recovery substudy analysis was performed in a subset of patients from the HERO study, which was not based on randomization. Therefore, results are not interpretable, and no statistical inference can be made.
Mean testosterone level in subgroup followed for testosterone recovery (N=184)1,3,5
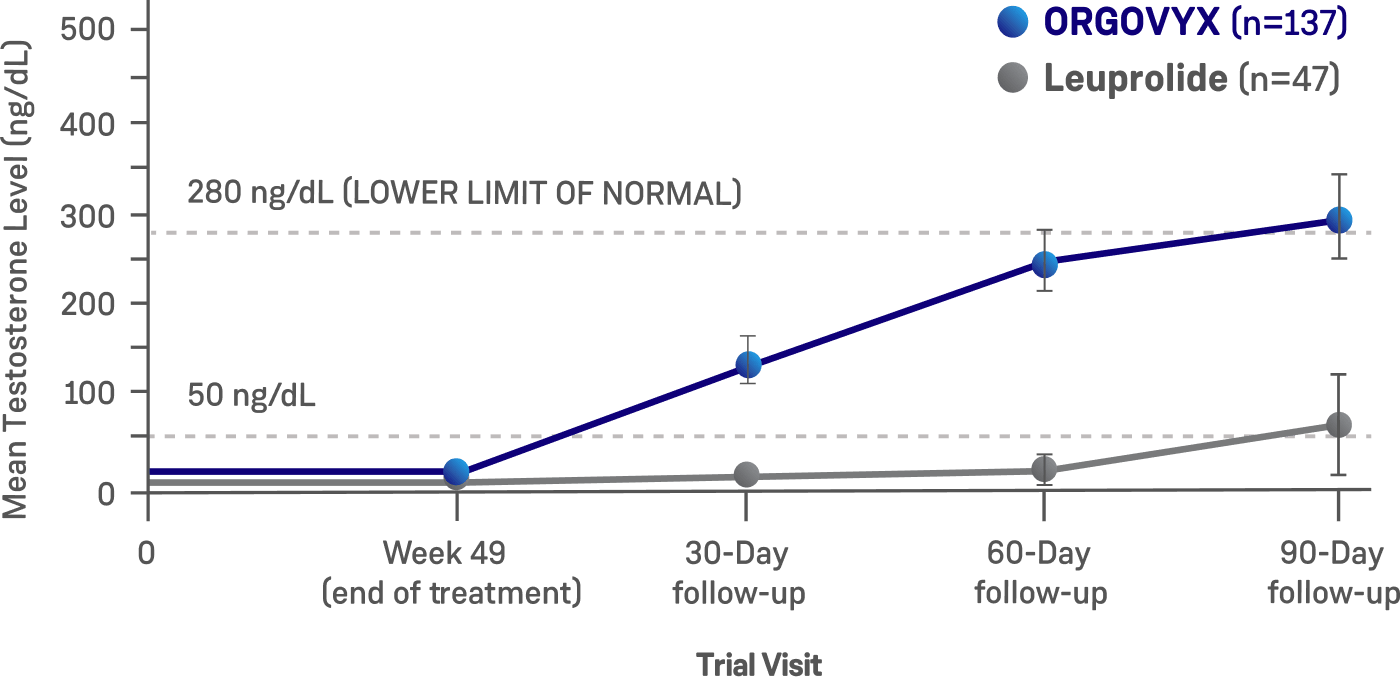
Adapted from: Shore ND, et al. New Engl J Med. 2020.
- Testosterone recovery was evaluated in a substudy of 184 patients who completed 48 weeks of treatment3,5
- 90 days after treatment discontinuation, 55% of 137 men treated with ORGOVYX had their testosterone levels return to above the lower limit of the normal range (>280 ng/dL) or baseline values1*
- 3% of 47 men treated with leuprolide had their testosterone levels return to above the lower limit of the normal range (>280 ng/dL) or baseline values 90 days after discontinuation3*
*Kaplan–Meier estimates within each group.1
Study Enrollment Criteria
The HERO study enrolled patients across different clinical disease presentations of advanced prostate cancer1
- Men with confirmed adenocarcinoma of the prostate
- ≥18 years of age
- At least one year of continuous ADT required with one of the following clinical disease presentations:
- Evidence of biochemical (PSA) or clinical relapse following local primary intervention with curative intent
- Newly diagnosed androgen-sensitive metastatic disease
- Advanced localized disease unlikely to be cured by local primary intervention with curative intent
- Serum testosterone ≥150 ng/dL
- Serum PSA >2.0 ng/mL*
- ECOG score 0/1
- Patients likely to require chemotherapy or surgical therapy for symptomatic disease management within 2 months of initiating ADT
- Previously received GnRH analog or other form of ADT for >18 months total duration
- If ADT was received for ≤18 months total duration, then patients must have completed treatment >3 months prior to baseline, or at least as long as the dosing interval of the depot formulation received
- Significant cardiovascular risk conditions
- Myocardial infarction or thromboembolic events within 6 months
- Arrhythmias
- Uncontrolled hypertension
Patients with disease progression during the treatment period, in the setting of testosterone suppression to castrate levels, were encouraged to remain on study and, if indicated, could receive radiotherapy as prescribed by the investigator. Concomitant radiotherapy was allowed no sooner than 2 months after initiating ADT. In the setting of rising PSA, patients could also receive enzalutamide after the confirmation of PSA progression. For patients requiring other systemic antineoplastic therapy during the treatment period, the investigator was encouraged to contact the medical monitor.4
When applicable, post radical prostatectomy of >0.2 ng/mL or post radiotherapy, cryotherapy, or high-frequency ultrasound >2.0 ng/mL above the post-interventional nadir.4
ECOG=Eastern Cooperative Oncology Group; GnRH=gonadotropin-releasing hormone.
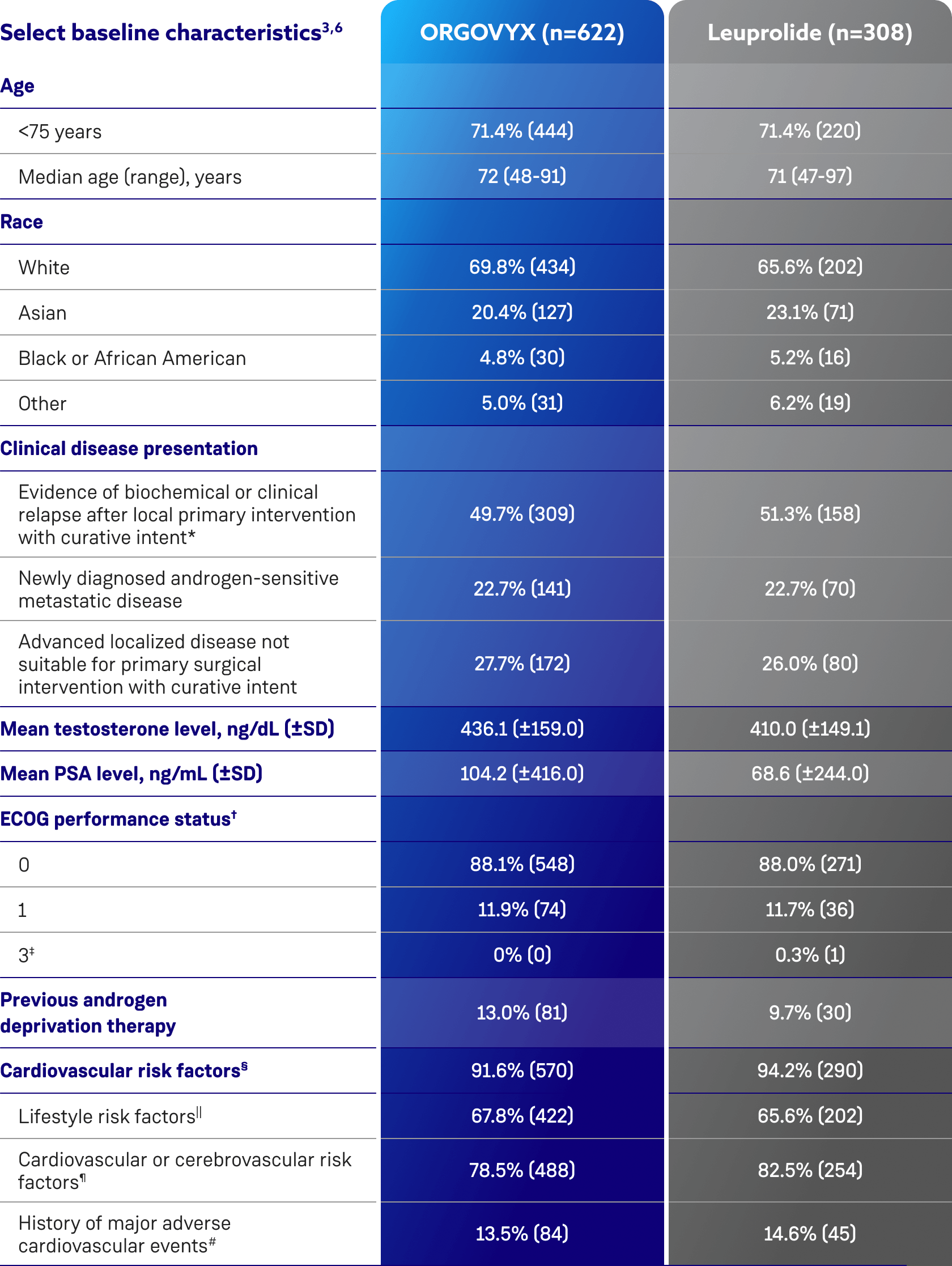
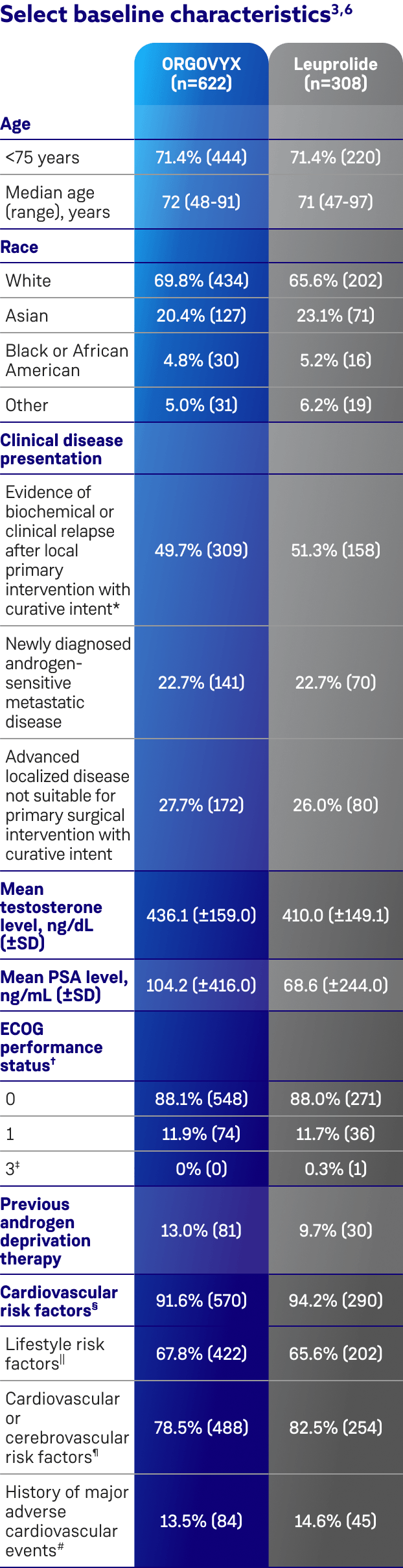
Baseline characteristics were well
balanced between treatment arms3,6
Patients on ORGOVYX with disease progression who received additional therapy1,7,8
- 16% (n=99) of patients on ORGOVYX received concomitant radiotherapy
- 2.7% (n=17) of patients on ORGOVYX received concomitant enzalutamide
- 1.3% (n=8) of patients on ORGOVYX received concomitant docetaxel
Biochemical relapse was defined by a rising PSA level.3
ECOG performance status ranges from 0 to 5, with higher scores reflecting greater disability.3
One patient in the leuprolide group had a surgical vascular procedure on his leg and was given an ECOG score of 3 at screening because of the use of crutches. By the baseline Day 1 visit, the patient no longer used crutches, and his ECOG score had improved to 0.3
Patients with multiple risk factors were counted only once.3
Included current/past tobacco smoking, heavy alcohol use, and a BMI >30 kg/m2.3
Included hypertension; dyslipidemia; diabetes; a history of myocardial infarction or CVD; a history of stroke, transient ischemic attack, or cerebral hemorrhage; peripheral arterial disease; atrial fibrillation and other arrhythmias; heart-valve disease; chronic obstructive pulmonary disease; chronic kidney disease; chronic liver disease; carotid artery stenosis or occlusion; venous thromboembolic events; and heart failure.3
Search criteria included "myocardial infarction" (broad standardized MedDRA query) and "central nervous system hemorrhages and cerebrovascular conditions" (broad standardized MedDRA query).3
BMI=body mass index; MedDRA=Medical Dictionary for Regulatory Activities; SD=standard deviation.
IMPORTANT SAFETY INFORMATION
Contraindication
ORGOVYX is contraindicated in patients with severe hypersensitivity to relugolix or to any of the product components.
Warnings and Precautions
QT/QTc Interval Prolongation: Androgen deprivation therapy, such as ORGOVYX may prolong the QT/QTc interval. Providers should consider whether the benefits of androgen deprivation therapy outweigh the potential risks in patients with congenital long QT syndrome, congestive heart failure, or frequent electrolyte abnormalities and in patients taking drugs known to prolong the QT interval. Electrolyte abnormalities should be corrected. Consider periodic monitoring of electrocardiograms and electrolytes.
Hypersensitivity: Angioedema was reported in 0.2% of patients treated with ORGOVYX in HERO. Hypersensitivity reactions, including pharyngeal edema and other serious cases of angioedema, have been reported post-marketing with ORGOVYX. Advise patients who experience any symptoms of hypersensitivity to temporarily discontinue ORGOVYX and promptly seek medical care. Discontinue ORGOVYX for severe hypersensitivity reactions and manage as clinically indicated.
Embryo-Fetal Toxicity: The safety and efficacy of ORGOVYX have not been established in females. Based on findings in animals and mechanism of action, ORGOVYX can cause fetal harm and loss of pregnancy when administered to a pregnant female. Advise males with female partners of reproductive potential to use effective contraception during treatment and for 2 weeks after the last dose of ORGOVYX.
Laboratory Testing: Therapy with ORGOVYX results in suppression of the pituitary gonadal system. Results of diagnostic tests of the pituitary gonadotropic and gonadal functions conducted during and after ORGOVYX may be affected. The therapeutic effect of ORGOVYX should be monitored by measuring serum concentrations of prostate-specific antigen (PSA) periodically. If PSA increases, serum concentrations of testosterone should be measured.
Adverse Reactions
Serious adverse reactions occurred in 12% of patients receiving ORGOVYX. Serious adverse reactions in ≥0.5% of patients included myocardial infarction (0.8%), acute kidney injury (0.6%), arrhythmia (0.6%), hemorrhage (0.6%), and urinary tract infection (0.5%). Fatal adverse reactions occurred in 0.8% of patients receiving ORGOVYX including metastatic lung cancer (0.3%), myocardial infarction (0.3%), and acute kidney injury (0.2%). Fatal and non-fatal myocardial infarction and stroke were reported in 2.7% of patients receiving ORGOVYX.
Most common adverse reactions (≥10%) and laboratory abnormalities (≥15%) in patients receiving ORGOVYX were hot flush (54%), glucose increased (44%), triglycerides increased (35%), musculoskeletal pain (30%), hemoglobin decreased (28%), alanine aminotransferase increased (27%), fatigue (26%), aspartate aminotransferase increased (18%), constipation (12%), and diarrhea (12%).
Drug Interactions
Co-administration of ORGOVYX with an oral P-gp inhibitor increases relugolix exposure, which may increase the risk of adverse reactions associated with ORGOVYX. Avoid co-administration of ORGOVYX with oral P-gp inhibitors. If co-administration is unavoidable, take ORGOVYX first and separate dosing by at least 6 hours. Monitor patients for increased adverse reactions. Treatment with ORGOVYX may be interrupted for up to 2 weeks if a short course of treatment with a P-gp inhibitor is required. Resume ORGOVYX after the P-gp inhibitor is discontinued. If treatment with ORGOVYX is interrupted for greater than 7 days, restart ORGOVYX with a 360 mg loading dose on the first day and continue with 120 mg once daily.
Co-administration of ORGOVYX with a combined P-gp and strong CYP3A inducer decreases relugolix exposure, which may reduce the effects of ORGOVYX. Avoid co-administration of ORGOVYX with combined P-gp and strong CYP3A inducers. If co-administration is unavoidable, increase the ORGOVYX dose to 240 mg once daily. After discontinuation of the combined P-gp and strong CYP3A inducer, resume the recommended ORGOVYX dose of 120 mg once daily.
Please see full Prescribing Information for ORGOVYX.
INDICATION
ORGOVYX® (relugolix) is a gonadotropin-releasing hormone (GnRH) receptor antagonist indicated for the treatment of adult patients with advanced prostate cancer.